Three Ways to Estimate COVID-19’s Real Toll in Africa
August 7 brought unwelcome news: the number of confirmed cases of COVID-19 in Africa had surpassed one million. Experts suspect even this eye-popping figure is a significant undercount.
Rich and well-resourced countries have struggled to come up with their own accurate coronavirus numbers. Most African countries are not wealthy, with fewer experts in tracking diseases at their disposal, and the volume and consistency of testing varies within and among these countries. When fewer people are tested, especially in more remote areas, many infections are likely to be missed.
Where does that leave us when trying to understand the true toll of COVID-19 on the African continent? Fortunately, there are ways to at least estimate a more realistic figure. We suspect the total is somewhere around 10 million. How did we arrive at that number?
Since we don’t have completely reliable data to go on, our estimates have to be based on assumptions. But we can be more confident by triangulating results from different methods. Here’s how it can be done, using three approaches to estimate the true number of COVID-19 infections in Africa:
1. The model approach
As of July 29, the University of Washington’s Institute for Health Metrics and Evaluation (IHME) estimated a total of 8.6 million COVID-19 cases across 41 countries in Africa (covering just over 1.2 billion people, or around 90% of the continent’s population). That estimate was 10 times the 877,000 confirmed cases reported by these countries by that date.
According to the IHME, the one million infections mark was already reached in late April. How does IHME arrive at its estimate? It uses a combination of statistical and epidemiological models and applies these to real-time data, incorporating factors relevant to the spread of coronavirus, such as population density, mobility, self-reported mask use, and self-reported contacts (more details are available on IHME’s website). So far, these models have performed better than most other ones in predicting levels of mortality due to COVID-19 — which brings us to our next approach.
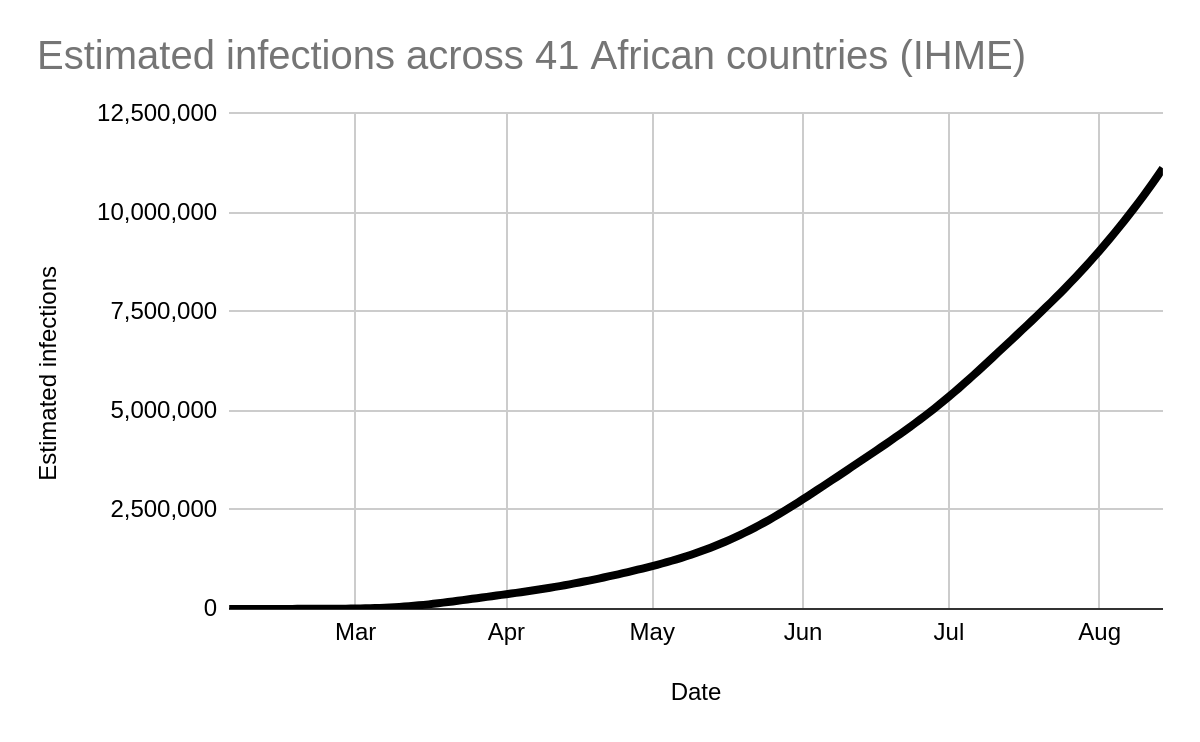
Estimated number of COVID-19 infections across 41 African countries. Source: IHME (as of August 12, 2020)
2. A matter of death and life
Another approach is to use the infection fatality rate (IFR) and the number of excess deaths to estimate the total number of people living with COVID-19. Using this logic, we arrive at an estimate of nine million infections across the African continent at the end of July, compared with 891,199 confirmed cases reported by Johns Hopkins University (JHU).
What does the IFR mean? It’s simply the proportion of people with a disease who die from it. For example, if we know that 1% of infected people end up dying in a region, and we see one death, we could fairly estimate that there have been 100 infections.
For COVID-19 in Africa, we projected the IFR at the regional and country levels, taking into account age, gender distribution, health-system quality, and comorbidities — all of which affect a person’s chance of survival. (For more information, see our methods section accompanying our Africa COVID-19 Community Vulnerability Index).
The predicted IFR for Africa as a whole is 0.55% — meaning that 0.55% of infected people will die, similar to estimates by others for low-income countries with limited healthcare capacity. The cumulative total number of deaths across Africa reported on July 29 by JHU — one of the most reliable sources for these figures — was 18,374. With an IFR of 0.55%, this translates to 3.3 million infections (18,375 / 0.0055).
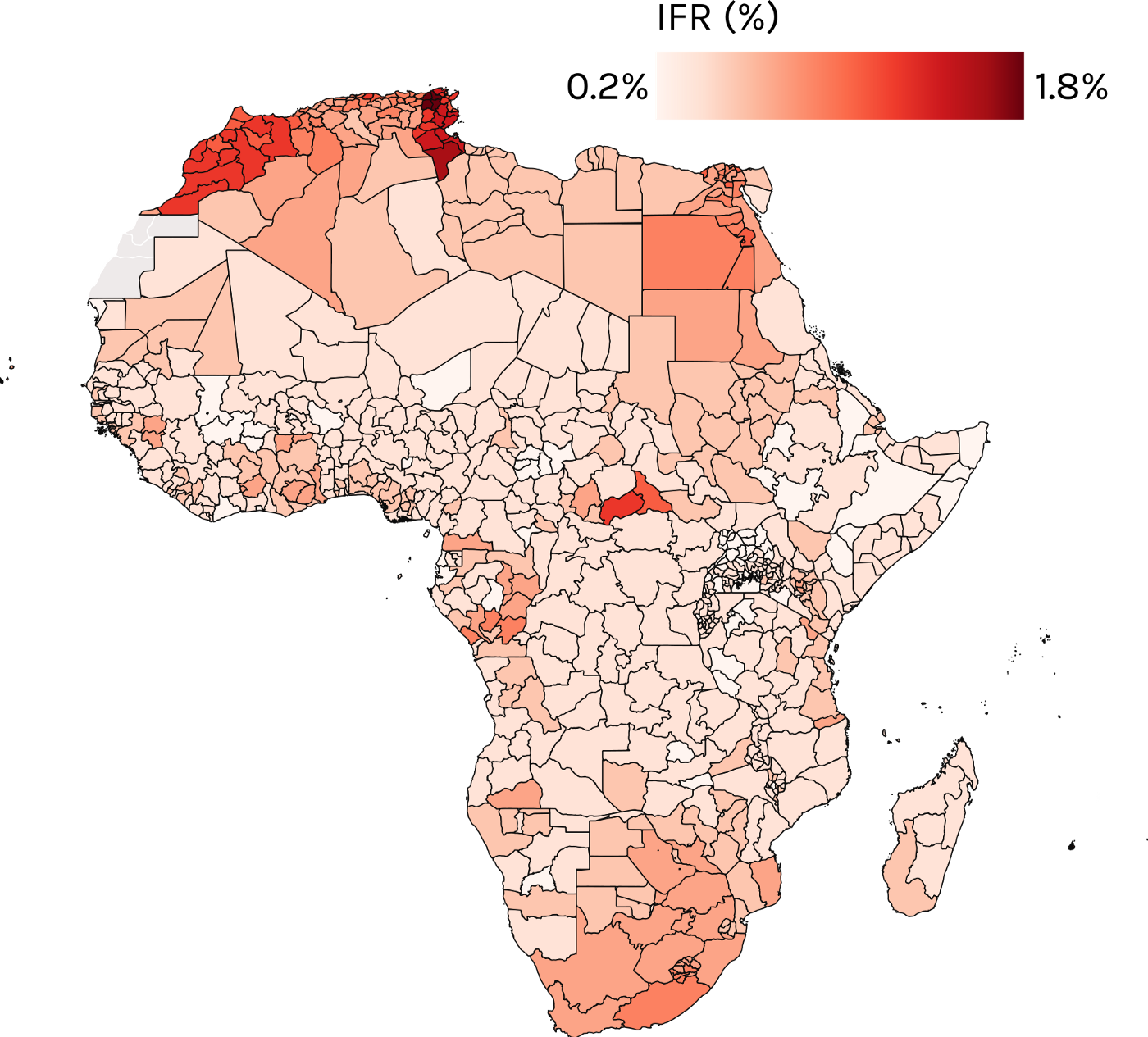
Predicted COVID-19 infection fatality rate. Source: Surgo Ventures.
But that’s not the end of the story — nor the calculation. (Bear with us: we promise the math is quite simple!) We know that deaths from COVID-19 are under-reported, because not every death due to the disease is classified as such. One common way of dealing with this discrepancy is to look at data on “excess deaths” — that’s the difference between the number of people who have died from any cause in a given period and the average number of deaths during the same period in recent years.
In the case of South Africa, for example, JHU reported 6,093 COVID-19 deaths from the beginning of the epidemic to July 23, but the South African Medical Research Council estimated that there had been 17,000 excess deaths during the same period. Since there’s no other apparent reason for these excess deaths, it suggests that for every death due to COVID-19, the true number of deaths is 2.8. Applying this multiplier to our earlier estimate of 3.3 million infections across the continent, we end up with an estimated 9.4 million infections (2.8 * 18,374 / 0.0055). This suggests we are underestimating the number of infections by nine times, close to IHME’s multiplier of 10.
Even this is optimistic, because South Africa has strong testing and is less likely to miss a COVID-19 death than most other countries. So in reality the multiplier may be greater than 2.8. It’s worth noting that this same calculation suggests that 2.2 million of these 9.4 million infections are in South Africa alone.
3. Testing the test data
In a number of US cities, studies of seroprevalence — the proportion of a population testing positive for a disease — by the US Centers for Disease Control and Prevention (CDC) have found that reported COVID-19 infections understate actual infections by a factor of roughly 10. Another study suggested a 9-times underestimation of infections in the US, due to inadequate testing rates and testing accuracy.

Test positivity rate across Africa as of August 12, 2020. Source: FinDX
Do we think Africa is missing more infections than the US? Tests in Africa have a positivity rate of ~11% (according to JHU and FindDX) compared to 7–8% in the US, which suggests that slightly more infections are going unnoticed in Africa. So the multiplier might go up from 10x somewhat, though it’s hard to say by how much.
Three methods, similar results
We can’t be sure how many people are infected with COVID-19 in Africa. But each of these approaches suggests more or less the same thing: the true number of infections may be around 10 million, even though the continent has only recorded one million confirmed cases.
It’s important to stress that each of the estimates we’ve discussed here comes with a large degree of uncertainty, and each method has its limitations. But triangulating methods helps give us confidence, especially when the estimates are not too far off from each other. And the upshot is clear: Africa needs — and deserves — the resources to address the pandemic and limit its further spread.
This work was made possible by everyone at the Surgo Ventures, including but not limited to (in alphabetical order): James Baer, Sofia Braunstein, Grace Charles, Anubhuti Mishra, Sema Sgaier, Peter Smittenaar, Nick Stewart, and Staci Sutermaster.
Technical Notes
For more information, see our methods section accompanying our Africa COVID-19 Community Vulnerability Index